Ulnar Nerve Compression at Guyon’s Canal by an Ulnar Artery Aneurysm: A Case Report

Article
Introduction
Ulnar nerve entrapment at the Guyon’s canal is a rare compression neuropathy of which the exact incidence and epidemiology are not clearly documented. Guyon’s canal is the fibro osseous tunnel at the wrist formed by pisiform bone medially, hook of hamate laterally, while transverse carpal ligament forms the floor, and the roof is formed by the volar carpel ligament. Both the ulnar artery and ulnar nerve run through the canal and the nerve divides into superficial sensory and deep motor branches. Clinical manifestations vary according to the site of the compression. The treatment principles of Guyon’s canal syndrome are that of other compression neuropathies. Potential structures causing the compression should be thought about before decompressive surgery.
Case Presentation
We report a case of Guyon’s canal syndrome due to an ulnar artery aneurysm subsequent to repetitive occupational trauma. A 35-year-old male presented with numbness over little and ulnar border of the middle finger for about 3 months period. Our patient is a mechanic working in a factory and the very first symptom he noticed was pain over the hypothenar eminence when using the screwdriver, about 1 year prior to the admission. The pain gradually increased over time both in intensity and frequency, but mostly at work. There was no visible abnormality of the hand, observed by the patient.
Over the last 3 months, he had developed numbness over the little and ring fingers and had accidental burns over the finger, following contact with hot metallic parts of machines. There was clumsiness in performing fine activities like fixing a screw. Mixing rice and food with the right hand was affected over the last month prior to admission.
On clinical examination, there was reduced sensation over the little and ulnar half of the ring finger and distal palm on the ulnar aspect. There was no demonstrable wasting of intrinsic muscles, but adduction and abduction of the fingers were weaker compared to the normal hand. The froment sign was weakly positive. There was tenderness over the hypothenar region with a positive Tinel sign.
Plain radiography of the wrist was unremarkable. Ultrasound scan demonstrated a vascular malformation within the thenar eminence, and the nerve conduction test confirmed compression of the ulnar nerve at the wrist.
The Allen test was performed before the operation and the palmar arches integrity was confirmed. At the surgical exploration opening the Guyon’s canal, a pulsatile, encapsulated lesion arising from the ulnar artery was found (Fig 1,2 ). This was about 2 x 2 cm and pressing on the ulnar nerve before the division of the deep branch. The ulnar nerve was dissected off the lesion and the cystic lump was excised ligating two ends of the ulnar artery (Fig 3). Hand perfusion was assessed and confirmed prior to ligation of the ulnar artery with microclamps applied proximal to the lesion on the artery.
Histology of the lesion revealed a cystically dilated vessel with a thinned-out muscular wall and a flattened endothelial lining. The lumen showed blood and fibrin, and the vessel wall showed myxoid change.
Discussion
Ulnar nerve entrapment at the Guyon’s canal is less common than at the elbow. Clinical manifestation varies with the level and duration of the compression. Aetiologically majority of ulnar nerve compressions at Guyon’s canal is idiopathic, identifiable lesions include ganglion cysts, hook of hamate fracture, tumours like lipoma, various vascular malformations, and abnormally located muscles[1,2,3]. Patient discussed in this case report clearly indicates repetitive trauma to the hypothenar area due to the frequent use of screwdrivers and other tools at his occupation. This could have initiated the formation of aneurysmal dilatation of the ulnar artery. Hence, our case could be a hypothenar hammer syndrome in which the ulnar nerve compression has occurred secondary to ulnar artery aneurysm at the Guyon’s canal.
Nerve conduction studies are used to confirm the clinical suspicion of ulnar nerve compression, and to identify the site of the compression. Nerve conduction studies are essential to evaluate concomitant carpal tunnel syndrome, C8, T1 radiculopathy and also peripheral neuropathy.
Basic imaging modality used in our case was Ultrasound scan that can visualise vascular anomalies in the region. Best imaging modality to evaluate a compressing lesion would be the MRI but in our case which was not done. Plain radiograph and USS scan are the essential radiological investigations and CECT and /or MRI should be done in selected cases to identify specific structural causes for the compressions[4,5].
In this case ulnar artery was not reconstructed as the perfusion of the hand was not affected following ligation of the artery. After the operation pain was relieved within 2- 3 days time. Hand movements and clumsiness of the hand movements were improved at 3 moths follow up and, he regained near normal sensation with good protective sensation. At one year follow up his hand was near normal and continue to do his usual work. Correct diagnosis and timely surgical decompression and abnormal structure pressing on the ulnar nerve should be removed appropriately. Undue delay should be minimised to preserve the complex function of the intrinsic muscles of the hand[6].

Figure 1: Intraoperative view of the ulnar artery aneurysm
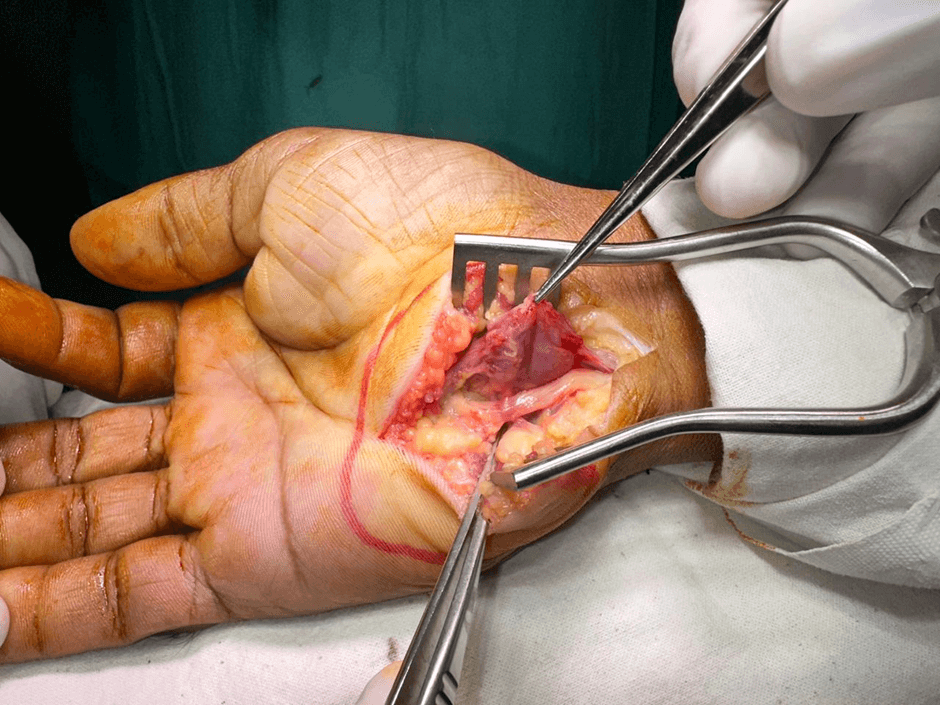
Figure 2: Ulnar artery aneurysm pressing on the ulnar nerve

Figure 3: Compressed segment of the ulnar nerve after excision of the aneurysm
Declarations
None
Ethics approval and consent to participate
Not applicable
Consent for publication
Informed written consent for publication and accompanying images was obtained from the patients prior to collecting information.
Availability of data and material
All data generated or analyzed during this study are included in this published article
Competing interests
The authors declare that they have no competing interests.
References
- Jae Hoon Lee , Jun-Ku Lee , Jin Sung Park. Characteristics of surgically treated Guyon canal syndrome: A multicenter retrospective study. J Plast Reconstr Aesthet Surg, 2022 Sep;75(9):3269-3278.
- Quang VP, Quoc HH, Guyon’s canal resulting from lipoma: A case report and review of the literature. Int J Surg Case Rep. 2022 Jun;95:107182
- Jiménez I, Manguila F, Dury M. Hypothenar hammer syndrome. A case report. Rev Esp Cir Ortop Traumatol. 2017 Sep-Oct;61(5):354-358.
- Hui-Chou HG, McClinton MA. Current options for treatment of hypothenar hammer syndrome. Hand Clin. 2015 Feb;31(1):53-62.
- Vasu Pai, Andrew Harp. Guyon’s canal syndrome: a rare case of venous malformation Hand Microsurg.2010 Jan 8;1(2):113-115.
- P Hoogvliet J H Coert, J Fridén. How to treat Guyon’s canal syndrome? Results from the European HANDGUIDE study: a multidisciplinary treatment guideline. Br J Sports Med . 2013 Nov;47(17):1063-70.