Scalp Angiosarcoma: A Case Report

Article
Introdcution
Angiosarcoma is an aggressive malignancy with a poor prognosis. The 10-year survival rates for scalp angiosarcoma range from 13.8% in cases with metastatic disease to a more favourable 53.6% when the tumour is localized[1]. Primarily affecting the face and scalp, angiosarcoma most commonly occurs in elderly individuals[2]. Its presentation is often deceptive, initially appearing as a benign lesion. However, it typically follows a highly aggressive course, with a significant risk of metastasis via lymphatic or hematogenous pathways. Early-stage treatment relies heavily on surgical excision, which remains the cornerstone of management. One of the most prevalent challenges, however, is the recurrence of the tumour following surgical intervention. But one of the most common problems is tumour recurrence following surgery[3].
Case presentation
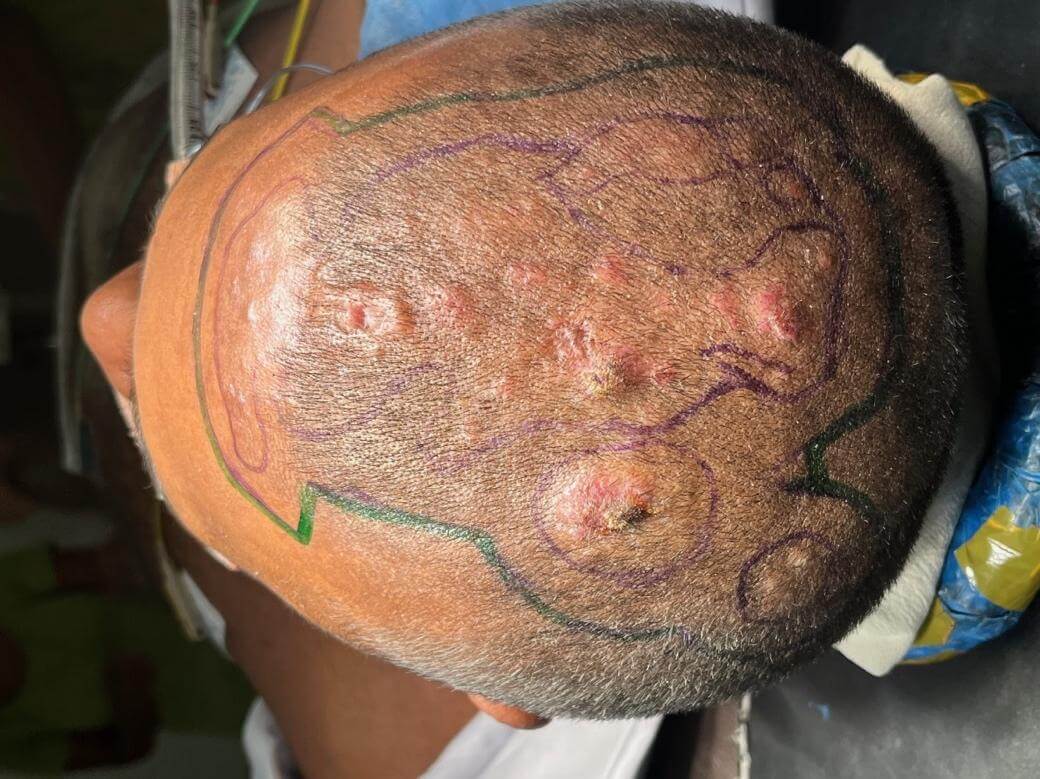
A 47-year-old male presented to the dermatology clinic with multiple asymptomatic scalp lesions in the left fronto-parietal region, persisting for 3 months. (20x18cm) On examination, an indurated erythematous nodular plaque with scaly satellite lesions were identified. A biopsy revealed a poorly demarcated dermal lesion characterized by numerous irregularly shaped, anastomosing vascular channels lined by atypical endothelial cells, consistent with a diagnosis of cutaneous angiosarcoma. Immunohistochemistry confirmed the diagnosis.
The patient was subsequently admitted and referred to the plastic surgery team. Given the widespread nature of the angiosarcoma, with multifocal lesions distributed across the scalp, a wide local excision followed by skin grafting was planned. The staging CT scan did not reveal any evidence of metastatic disease.
One and a half months after the diagnosis, the patient underwent wide local excision of the scalp, with intraoperative frozen sections used to assess margin clearance. An initial resection margin of 2 cm was taken, but frozen section analysis revealed a positive deep margin. As a result, an additional 2 cm of tissue was resected which was also positive. Due to the unavailability of a frozen section facility after hours, a further 1 cm margin was excised and sent for histopathological examination. The resulting skin defect was covered with a split-thickness skin graft. Unfortunately, the final resection margin was still positive on the histopathology report.
The patient was initially scheduled for re-resection, but the procedure was delayed due to MRSA colonization of the wound. After successful decolonization, the re-resection was performed approximately one month after the initial intervention.
During the re-resection, the outer table of the skull was burred, and an additional 2 cm margin was excised. Intraoperative frozen section analysis confirmed clear margins, with no residual tumour deposits. However, due to time constraints in the operating theatre, the definitive reconstruction was postponed.
The final reconstruction was subsequently carried out. Another 0.5 cm margin was removed, and the outer table of the skull was reburred. The defect was then covered with a latissimus dorsi flap, and a split-thickness skin graft. During the procedure, the right superficial temporal artery and vein were exposed, and the latissimus dorsi muscle flap was raised. The artery and vein of the flap were anastomosed with the superficial temporal artery and vein. The exposed bone was covered with the muscle flap and secured using 2-0 Vicryl sutures. A meshed split-thickness skin graft was placed on the muscle flap.
The patient experienced an uneventful recovery, with no complications such as hematoma, infection, or flap failure. On postoperative day 7, the skin graft was inspected, showing 95% graft take. The patient was subsequently discharged on postoperative day 8. A follow-up appointment was scheduled for one-week post-discharge, with additional monthly follow-ups planned. The patient also expressed a willingness to use a hair wig moving forward the surgical outcome was aesthetically acceptable.
Discussion
Angiosarcoma arises from the differentiation of vascular or lymphatic endothelial cells, constituting around 1%–2% of all soft tissue sarcomas[4]. Among head and neck soft tissue sarcomas, it exhibits the highest propensity for lymph node metastasis, with distant metastases occurring in up to 50% of cases. The lungs are the most frequent site of metastasis, followed by the liver[5]. Clinically, angiosarcoma often begins as a bluish discolouration, but its presentation can vary widely, ranging from asymptomatic lesions to those showing necrosis and crust formation, often accompanied by bleeding[6]
A definitive diagnosis may be delayed in cases with nonspecific symptoms, as conservative management is often pursued without a biopsy. This delay in diagnosis and subsequent treatment can significantly reduce survival rates. Immunohistochemistry plays a critical role in both the diagnosis and the differential diagnosis of angiosarcoma, offering valuable insights for early detection and treatment planning[6].
Various treatment approaches are available, including radiotherapy, chemotherapy, cytokine therapy, and wide local excision. Radiotherapy has been shown to improve survival rates, particularly in patients with multifocal lesions. While the efficacy of chemotherapy remains a subject of debate, paclitaxel has emerged as a promising advancement in therapeutic strategies. Cytokine therapy, involving intralesional interferon alpha-2b and interleukin-2 combined with surface radiotherapy, has been explored as an alternative to surgery. For early-stage tumours, wide local excision remains the preferred treatment. In this case, given the prompt diagnosis, wide local excision was the most suitable option[7].
Given the aggressive nature of angiosarcoma, wide local excision often results in large defects with exposed bone. Several reconstructive techniques are available, including skin grafts, free flaps and the use of skin substitutes[8]. Gudewer et al reported successful scalp reconstruction using a free muscle flap and skin graft following angiosarcoma resection, with both functional and aesthetic outcomes being satisfactory[9].
Skin grafting is a feasible option for reconstruction following wide local excision, but it should only be performed once granulation tissue has sufficiently developed at the surgical site. However, the formation of granulation tissue can be time-consuming, increasing the risk of surgical site infection during this period. Patients often express dissatisfaction with this approach, as it necessitates prolonged exposure to an open wound, leading to extended hospital stays.
Dermal alternatives offer another viable option for reconstruction. Skin substitutes are a diverse group of biological, synthetic, or biosynthetic materials designed to provide either temporary or permanent coverage for open skin wounds. Ideally, these substitutes mimic the composition and function of natural skin or facilitate autologous regenerative healing when applied to a wound. Examples include Integra® (LifeScience Corp., Plainsboro, NJ, USA) and NovoSorb® BTM (Biodegradable Temporizing Matrix, PolyNovo Biomaterials Pty Ltd). However, NovoSorb® BTM is currently unavailable in Sri Lanka, and the use of Integra® is impractical for larger skin defects due to its high cost.
Free tissue transfer flaps play a crucial role in such reconstructions. Flaps can be muscle flaps or fasciocutaneous flaps. Fasciocutaneous flaps have the disadvantage of donor site morbidity due to their large size in this case. And the appearance can be bulky. Muscle flaps are a better option for this patient. Studies recommend the latissimus dorsi flap, anterolateral thigh (ALT) flap, and radial forearm flap as primary reconstructive options. The ALT flap has gained popularity due to its low donor site morbidity and ease of harvest, while the radial forearm flap’s major limitation is the restricted size of the available tissue at the donor site[8].
The latissimus dorsi flap is often favoured for reconstruction due to its large size, making it an ideal candidate. Additionally, its vascular pedicles offer compatible calibres and sufficient length, particularly when compared to the superficial temporal vessels. In this case, a split-thickness skin graft was applied over the muscle flap, as studies suggest faster secondary healing occurs when a muscle flap supports the graft[10].
Some studies have identified donor-site morbidity as a disadvantage of latissimus dorsi muscle transfer, particularly noting reduced shoulder function due to extensive muscle resection. This is most evident in the early postoperative period, with patients experiencing weakened shoulder strength, especially during extension, internal rotation, and adduction movements[11].
Conclusion
Scalp angiosarcomas is a rare highly aggressive cutaneous malignancy with poor prognosis. Wide local excision is the preferred option for early-stage tumors. Lattismus dorsi flap is a good reconstructive option due to its large size and vascular compatibility. The split-thickness skin graft performed over the muscle flap has better healing with a cosmetically appealing result.









Consent
Informed written consent was obtained from the patient for publication, inclusive of images.
Ethical Approval
Not applicable
Competing interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
None
References
-
J. Albores-Saavedra, A. M. Schwartz, D. E. Henson et al., “Cutaneous angiosarcoma. Analysis of 434 cases from the surveillance, epidemiology, and end results program, 1973–2007,” Annals of Diagnostic Pathology, vol. 15, no. 2, pp. 93–97, 2011.
-
Pawlik TM, Paulino AF, McGinn CJ, et al.: Cutaneous angiosarcoma of the scalp: a multidisciplinary approach. Cancer. 2003, 98:1716-26. 10.1002/cncr.11667
-
Young RJ, Brown NJ, Reed MW, Hughes D, Woll PJ: Angiosarcoma. Lancet Oncol. 2010, 11:983-91.
-
Lee KC, Chuang SK, Philipone EM, Peters SM. Characteristics and prognosis of primary head and neck angiosarcomas: A Surveillance, Epidemiology, and End Results Program (SEER) analysis of 1250 cases. Head and Neck Pathology [Internet]. 2018 Oct 24;13(3):378–85. Available from: https://doi.org/10.1007/s12105-018-0978-3
-
Patel SH, Hayden RE, Hinni ML, Wong WW, Foote RL, Milani S, et al. Angiosarcoma of the scalp and face. JAMA Otolaryngology–Head & Neck Surgery [Internet]. 2015 Apr 1;141(4):335. Available from: https://doi.org/10.1001/jamaoto.2014.3584
-
Near total-Choi SY, Baek IS, Park CG, Hong IP. Near total excision in patients with Angiosarcoma on scalp. Journal of Korean Society of Plastic and Reconstructive Surgery [Internet]. 2011(38): 711-714.
-
4. Miqueloti MB, Gonzaga CB, Da Silva Azambuja Ribeiro V, Filho EG, Freire RAV. Scalp reconstruction after wide resection of an angiosarcoma. Revista Brasileira De Cirurgia Plástica [Internet]. 2019 Jan 1;34(4). Available from: https://doi.org/10.5935/2177-1235.2019rbcp0239
-
Chou PY, Kao D, Denadai R, Huang CY, Lin CH, Lin CH. Anterolateral thigh free flaps for the reconstruction of scalp angiosarcoma – 18-year experience in Chang Gung memorial hospital. Journal of Plastic Reconstructive & Aesthetic Surgery [Internet]. 2019 Dec 1;72(12):1900–8. Available from: https://doi.org/10.1016/j.bjps.2019.07.024
-
Gudewer E, Hölzle E, Li L. Widespread cutaneous angiosarcoma of the scalp: diagnosis and soft tissue reconstruction with a combined double-muscle-free flap and split-thickness-skin graft. Oral and Maxillofacial Surgery [Internet]. 2009 Mar 19;13(2):95–8. Available from: https://doi.org/10.1007/s10006-009-0147-7
-
Choi JH, Ahn KC, Chang H, Minn KW, Jin US, Kim BJ. Surgical treatment and prognosis of angiosarcoma of the scalp: a retrospective analysis of 14 patients in a single institution. BioMed Research International [Internet]. 2015 Jan 1;2015:1–8. Available from: https://doi.org/10.1155/2015/321896
-
Lee SH, Lee KT. Reconstruction of extensive scalp defects of oncologic origin using thoracodorsal artery perforator free flaps. Archives of Hand and Microsurgery [Internet]. 2023 Nov 10;28(4):287–95. Available from: https://doi.org/10.12790/ahm.23.0025